History of Psychodynamic Therapy
"Viennese Culture and its Psychological Complexities"
By Sinthia Cousineau
Vienna is well-known as the home of the famous Sigmund Freud the founder of psychoanalytic theory. He developed the therapeutic techniques that are still implemented in therapy today, such as the use of free association and transference. He was also very interested in how sexuality affects one’s mind in particular how the sex drive can affect the death drive. He developed the theory of the unconscious and divides the mind into three psychic structures known today as the id, ego, and super ego. Freud was born in Austria on May 4th, 1856 and studied in the University of Vienna. Today he is one of the most mentioned names in the field of psychology. Psychoanalysis was thus born in Vienna due to his work in the field of mental illness. However the city of Vienna had long been affected by an interest in mental illness prior to Freud’s time. This paper will focus on how the introspection tendencies were characteristic of Viennese culture during the late-nineteenth and early twentieth centuries. It will also explore why introspection tendencies were characteristic of Viennese culture. Vienna has been interested in mental illness and problems of sexuality long before Freud. In fact Freud is not the only contributor to this field, there were many who before before him. According to Bettleheim (1990) Vienna had many other contributors to the field of mental illness prior to Freud. For instance Baron Richard von Krafft-Ebing, a professor at the University of Vienna who first gave name to paranoia, and explored the many forms of sexual drive in his “Psychopathia Sexualis” published in 1886 which revolutionaries the way the world viewed sexual perversions. This is turn led to the decriminalization of sexual perversions in Austria and thus led to an era of changed attitudes regarding sexuality in Vienna. Vienna also had other contributors to the field of mental illness such as Wagner von Jouregg, the head of the psychiatry department at the University of Vienna who won a Noble prize in medicine in 1927 for his work was the begging of chemical treatment for mental illness. Another physician, Manfred Sakel also from Vienna, discovered the insulin-shock treatment for schizophrenia in 1933.
To better understand Vienna’s interest in mental illness one needs to understand its history as well. Bettleheim (1990) states that Vienna was once called “die alte kaiserstadt” which meant “the old imperial city”. Vienna was once the capital of the Hapshurg Empire, who at one point in time was far greater than even the famous Roman Empire. This Empire started to decline in power in the 16th century when its emperor Charles V couldn’t make claim. There was a revolution in 1848 that lead to the forced resignation of Prince Metternich (Austria’s chancellor) this lead to the beginning of the reign of Franz Joseph an emperor who’s history is stained by mental illness and tragedy that would not only affect Vienna but the entire world as well. During this time of history Vienna became very multicultural after the Napoleonic wars, it was once the seat of the empire where most of the important cultural institutions where in its influence. Vienna was also the second largest city in Europe, after Paris.
Its history was particularly affected in 1866 when Prussia became the dominant power. After the war with Prussia, Austria was no longer the dominant power over the other German states. In 1870 after Prussia defeated France, Berlin would replace Vienna as the center of the Garman-speaking world. Bettleheim (1990) states that due to this Vienna would turn to denial as a kind of defense, and would begin focusing more on mental illness then the world itself: “External Reality is discounted and all mental energy is turned inward” only the inner life of the individual is allowed to matter” (Bettleheim, 1990, p.7). While German was focusing on building its empire, Vienna’s cultural elites would focus on discovering and conquering the inner world of man. Conquering mental illness was part of this new focus. Vienna was both an old imperial capital and a center for modern culture.
Emperor Franz Joseph began Vienna’s preoccupation with mental illness the moment he marries Elizabeth, a young and beautiful Bavarian princess. She was once considered the most beautiful women in Europe however history would describe her as hysterical, narcissistic and anorexic. She was known to starve herself, drinking nothing but six glasses of milk per day. Part of her neurosis involved her endlessly and aimlessly traveling all over Europe. When the emperor asked her what she wanted for her name day she replied “what I would really like best would be a completely equipped insane asylum” (Bettleheim, 1990, p. 9). In fact madness was very common in her family so she frequently visited institutions deigned for the insane. She was then assassinated by an anarchist in 1898 when traveling on one of her lavish trips to Geneva. Considering Vienna’s history it was clear that an interest in insanity and the devastating impact of neurosis and hysteria was found in the imperial court which dominated Vienna long before Freud’s time. Another example regarding this is Rudolf, the son of Emperor Franz Joseph and Elisabeth. He lead a very lonely lifestyle, became very depressed and seeking comfort in many the affairs he had with women. He was not very close to his father and his mother never showed him much attention. Due to his distant and unavailable mother he developed an oedipal complex, with his sex drive eventually leading to murder and suicide when he would eventually kill himself and his lover in a suicide pact. This shows a possible connection in the relationship between sex drive and the death drive which would later be explored by Freud. After his son’s death the Emperor had difficulty coping and developed work neurosis. Rudolf’s deaths lead Elisabeth to obsess about maintaining her beauty and youth, she would withdraw from court life and travel endlessly. After this tragic story in the imperial court the Emperor having lsot his only son and heir names Archduke Francis Ferdinand as the next ruler. He was eventually assassinated in 1914 and thus beginning the events leading to the First World War.
Since these events that marked history, Vienna’s culture have a strong interconnection between sex and death, which would form a major topic for most of its art forms such as its art and literature. For instance Bettleheim (1990) describes an incident when in 1881 Vienna’s Ring Theater burnt down resulting in great loss of life. The emperor decreed that this tragic site become a new residential building called “house of atonement” which would charge high rents to help support the orphaned children of this tragedy. At least people were reluctant to live there because of the death that occurred on the site. Freud however, once he married decided to move in that location. He even received a letter from the emperor himself to congratulate him on his first child being the first to be born in that building. Freud believed that the strongest inner powers were the thanatos, eros, death and sex. His alter ego was the well-known Viennese literary figure Arthur Schinizler, who also studied the man’s psyche. He wrote two plays titled “A little Love Affair” and “Enormous Country”. Both plays address the topic of sexual affairs that eventually results to death either by dual or suicide. His novel “Miss Else” also addresses this theme of sexual involvement leading to destruction.
One decade after Elizabeth’s death, Vienna built an institution to house the insane. Its architect was Otto Wagner and it was the Church of St. Leopold at Steinhof. A place devoted to serving people suffering from mental illness. It was a true work of art. “During the last years of the disintegration of the great Hapsburg Empire, it’s capital paid tribute to the importance of madness with a beautiful and impressive monument” (Bettleheim, 1990, p.16). Hence to understand Vienna’s interest in introspection in the ninetieth and twentieth century one needs to understand it’s history and how it was stained by tragedy related to mental illnesses and the psyche forces that drive it.
Reference
Bettleheim, B. (1990). Freud’s Vienna. Freud’s Vienna and other essays (pp. 1-23). New York, NY: Knopftit.
By Sinthia Cousineau
Vienna is well-known as the home of the famous Sigmund Freud the founder of psychoanalytic theory. He developed the therapeutic techniques that are still implemented in therapy today, such as the use of free association and transference. He was also very interested in how sexuality affects one’s mind in particular how the sex drive can affect the death drive. He developed the theory of the unconscious and divides the mind into three psychic structures known today as the id, ego, and super ego. Freud was born in Austria on May 4th, 1856 and studied in the University of Vienna. Today he is one of the most mentioned names in the field of psychology. Psychoanalysis was thus born in Vienna due to his work in the field of mental illness. However the city of Vienna had long been affected by an interest in mental illness prior to Freud’s time. This paper will focus on how the introspection tendencies were characteristic of Viennese culture during the late-nineteenth and early twentieth centuries. It will also explore why introspection tendencies were characteristic of Viennese culture. Vienna has been interested in mental illness and problems of sexuality long before Freud. In fact Freud is not the only contributor to this field, there were many who before before him. According to Bettleheim (1990) Vienna had many other contributors to the field of mental illness prior to Freud. For instance Baron Richard von Krafft-Ebing, a professor at the University of Vienna who first gave name to paranoia, and explored the many forms of sexual drive in his “Psychopathia Sexualis” published in 1886 which revolutionaries the way the world viewed sexual perversions. This is turn led to the decriminalization of sexual perversions in Austria and thus led to an era of changed attitudes regarding sexuality in Vienna. Vienna also had other contributors to the field of mental illness such as Wagner von Jouregg, the head of the psychiatry department at the University of Vienna who won a Noble prize in medicine in 1927 for his work was the begging of chemical treatment for mental illness. Another physician, Manfred Sakel also from Vienna, discovered the insulin-shock treatment for schizophrenia in 1933.
To better understand Vienna’s interest in mental illness one needs to understand its history as well. Bettleheim (1990) states that Vienna was once called “die alte kaiserstadt” which meant “the old imperial city”. Vienna was once the capital of the Hapshurg Empire, who at one point in time was far greater than even the famous Roman Empire. This Empire started to decline in power in the 16th century when its emperor Charles V couldn’t make claim. There was a revolution in 1848 that lead to the forced resignation of Prince Metternich (Austria’s chancellor) this lead to the beginning of the reign of Franz Joseph an emperor who’s history is stained by mental illness and tragedy that would not only affect Vienna but the entire world as well. During this time of history Vienna became very multicultural after the Napoleonic wars, it was once the seat of the empire where most of the important cultural institutions where in its influence. Vienna was also the second largest city in Europe, after Paris.
Its history was particularly affected in 1866 when Prussia became the dominant power. After the war with Prussia, Austria was no longer the dominant power over the other German states. In 1870 after Prussia defeated France, Berlin would replace Vienna as the center of the Garman-speaking world. Bettleheim (1990) states that due to this Vienna would turn to denial as a kind of defense, and would begin focusing more on mental illness then the world itself: “External Reality is discounted and all mental energy is turned inward” only the inner life of the individual is allowed to matter” (Bettleheim, 1990, p.7). While German was focusing on building its empire, Vienna’s cultural elites would focus on discovering and conquering the inner world of man. Conquering mental illness was part of this new focus. Vienna was both an old imperial capital and a center for modern culture.
Emperor Franz Joseph began Vienna’s preoccupation with mental illness the moment he marries Elizabeth, a young and beautiful Bavarian princess. She was once considered the most beautiful women in Europe however history would describe her as hysterical, narcissistic and anorexic. She was known to starve herself, drinking nothing but six glasses of milk per day. Part of her neurosis involved her endlessly and aimlessly traveling all over Europe. When the emperor asked her what she wanted for her name day she replied “what I would really like best would be a completely equipped insane asylum” (Bettleheim, 1990, p. 9). In fact madness was very common in her family so she frequently visited institutions deigned for the insane. She was then assassinated by an anarchist in 1898 when traveling on one of her lavish trips to Geneva. Considering Vienna’s history it was clear that an interest in insanity and the devastating impact of neurosis and hysteria was found in the imperial court which dominated Vienna long before Freud’s time. Another example regarding this is Rudolf, the son of Emperor Franz Joseph and Elisabeth. He lead a very lonely lifestyle, became very depressed and seeking comfort in many the affairs he had with women. He was not very close to his father and his mother never showed him much attention. Due to his distant and unavailable mother he developed an oedipal complex, with his sex drive eventually leading to murder and suicide when he would eventually kill himself and his lover in a suicide pact. This shows a possible connection in the relationship between sex drive and the death drive which would later be explored by Freud. After his son’s death the Emperor had difficulty coping and developed work neurosis. Rudolf’s deaths lead Elisabeth to obsess about maintaining her beauty and youth, she would withdraw from court life and travel endlessly. After this tragic story in the imperial court the Emperor having lsot his only son and heir names Archduke Francis Ferdinand as the next ruler. He was eventually assassinated in 1914 and thus beginning the events leading to the First World War.
Since these events that marked history, Vienna’s culture have a strong interconnection between sex and death, which would form a major topic for most of its art forms such as its art and literature. For instance Bettleheim (1990) describes an incident when in 1881 Vienna’s Ring Theater burnt down resulting in great loss of life. The emperor decreed that this tragic site become a new residential building called “house of atonement” which would charge high rents to help support the orphaned children of this tragedy. At least people were reluctant to live there because of the death that occurred on the site. Freud however, once he married decided to move in that location. He even received a letter from the emperor himself to congratulate him on his first child being the first to be born in that building. Freud believed that the strongest inner powers were the thanatos, eros, death and sex. His alter ego was the well-known Viennese literary figure Arthur Schinizler, who also studied the man’s psyche. He wrote two plays titled “A little Love Affair” and “Enormous Country”. Both plays address the topic of sexual affairs that eventually results to death either by dual or suicide. His novel “Miss Else” also addresses this theme of sexual involvement leading to destruction.
One decade after Elizabeth’s death, Vienna built an institution to house the insane. Its architect was Otto Wagner and it was the Church of St. Leopold at Steinhof. A place devoted to serving people suffering from mental illness. It was a true work of art. “During the last years of the disintegration of the great Hapsburg Empire, it’s capital paid tribute to the importance of madness with a beautiful and impressive monument” (Bettleheim, 1990, p.16). Hence to understand Vienna’s interest in introspection in the ninetieth and twentieth century one needs to understand it’s history and how it was stained by tragedy related to mental illnesses and the psyche forces that drive it.
Reference
Bettleheim, B. (1990). Freud’s Vienna. Freud’s Vienna and other essays (pp. 1-23). New York, NY: Knopftit.

The Therapeutic Frame of Psychodynamic Psychotherapy
By Sinthia Cousineau
The psychodynamic theory focuses primarily on unlocking the past or the unconscious mind of the patient. Psychotherapy is therefore a form of treatment that aims to understand a patient’s unconscious, a concept originated by Freud who aimed to create a form a treatment that involves talking with a trained professional, hence the therapist. Cabaniss (2011) describes this understanding of the unconscious as “understanding what lies beneath the surface”. Once a patient understands and is made aware of their unconscious Cabaniss describes this as “uncovering”. For this to happen, the art therapist should establish an appropriate therapeutic frame for the psychotherapy, to allow the therapist to “separate what goes on in the therapy from what goes on outside” (Cabaniss, 2011, p.73). Art therapy is a field that uses art materials within the framework of a psychotherapeutic relationship. An art therapist uses the images that the patient produced to explore the unconscious of the patient for it allows the patient to focus on the issues and concerns that led them to start therapy (Dalley, 2013). This paper focuses on what constitutes the therapeutic frame in the field of psychotherapy and art therapy as well as describe why the establishment of the therapeutic frame is essential to this type of therapy. This is important because the therapy space is a place in which the patient will reveal their emotions, pain, vulnerabilities and personal tragedies. Hence, it is important for the patient to feel they are in a safe place to allow them to explore their unconscious mind and relive these emotions and painful childhood memories associated to these emotions. That is why patients need to be assured of the safety of the therapeutic setting (Cabaniss, 2011, p.73).
Cabaniss (2011) describes the therapeutic frame as being essential to the psychotherapy practice because it establishes a boundary for the therapist and patient as well as setting up a safe relationship for the patient. It also establishes a contract for the treatment that gives an idea of what to expect from the psychotherapy (Cabaniss, 2010). She describes how the frame of psychotherapy incorporates many different aspects such as the following: roles, time, setting, money, contact information, what to do in the event of an emergency, rules of confidentiality and issues related to supervision if the session is held by a therapist in training. Mainly Cabaniss focuses on how the frame of psychotherapy’s main purpose is to set a boundary which determines the appropriate behavior for therapist and patient. She describes it as being essential that that therapeutic frame be established at the start of therapy to help establish that boundary. She states that elements of the frame of psychotherapy should be considered the “ground rules” of psychotherapy. She also describes the two types of boundaries in psychotherapy. The first one is "boundary crossing which Cabaniss defines as a “deviation from the frame that may advance treatment and doesn’t harm the patient”. The second is boundary violation, which is “a deviation from the frame that is harmful or exploitative to the patient” (Cabaniss, 2011, p.72). This last one could be avoided by actively creating a frame with the patient.
The establishment of a therapeutic frame is essential to psychotherapy because it separates the outside world from what goes on in therapy, which enables the client to be assured they are in a safe space. Cabaniss (2011) also states that it allows a standard way for all patients meaning that each patient will be treated with the same elements of the therapeutic frame hence the same environment for their art making, the same rules of the patient-therapist relationship apply, and same boundaries. Role, a crucial element of the therapeutic frame is described as a part or function that a person plays in a particular situation. Cabaniss (2011). The role has two different parts: function and responsibilities. These are different for the therapist and the patient, for example the role of the art therapist or any psychotherapist is to listen to the patient, be understanding and nonjudgmental as to create a safe space for the patient and to be reliable by always showing up on time or alerting patient if late. The role of the patient is to attend the sessions on time, pay for the sessions and speak and participate in these sessions. When setting the frame both therapist and patient acknowledge which behavior is not appropriate, such as physical contact between therapist and patient. The patient should also be made aware that harassing the therapist is inescapable while the therapist however should avoid answering personal question as not to reveal too much about themselves to their client. As too much personal information will change the therapeutic relationship. Theses boundaries allow the session to become a safe place in which thoughts and feelings are allowed to surface (Dalley, 2013, p.8). Another important element of the therapeutic frame is time. According to Cabaniss (2011), setting a time allows the therapist to protect their patient. It means setting a time for individual sessions, a schedule of sessions and an overall ideal as to the duration of the therapy itself. The time should be reasonable for both patient and therapist. A third element of the therapeutic frame and one of the more important ones is the setting of the therapy. According to Cabaniss it is essential that the setting be a place designed for psychotherapy such as a clinic room or private office. Having the therapy session at a Starbucks for instance is not a good idea because it would turn the session into a social interaction, when therapy itself should remain a professional agreement. The setting also plays a crucial role in protecting the triatic relationship of therapist, patient and psychotherapy because it allows a safe space for the client to explore their unconscious. Cabaniss (2011) emphasizes the important of a “comfortable setting” which is a place where the patient is not bombarded with the personal information of the therapist. For example an office filled with photos of the therapist’s family or vacation trips would not be suitable. Other elements of the therapeutic frame include money. For therapy is a professional agreement and the client pays for the service of a professional. If for instance a patient cannot afford therapy the therapist should try to help them find a therapeutic service they could afford. Knowing the budget of the patient would also help establish how many sessions they could afford. Another element is the confidentiality of contact information. According to Cabaniss (2011) there are two reasons why a patient may need to contact their therapist outside of their session, and those are in the event of an emergency or to convey information such as needing to change the time of the session. Cabaniss also recommends that therapist have a separate phone line for their practice as to avoid mixing their professional life with their personal life. Transference is a very important concept in psychotherapy. It is described by Dalley (2013) as feelings that originate from childhood experiences or memories onto the therapist. Art making allows a patient to relive these memories and feelings. Based on Dalley’s description of Kim’s experience with Gabriella, we can see this surface as Kim is reliving his earlier memories of his parent’s fighting and sister’s eating disorder and his distant brothers. Making unconscious processes conscious is very complex and is achieved through interpretation of an image. This is how the art therapist facilitates communication and exploration of the unconscious by allowing the patient to create and then interpret their work (Dalley, 2013, p. 10). For example when interpreting Kim’s drawing of himself repairing his car, we can see that he was shutting himself off from society as he drew himself with his back turned to us and the hood of his car shielding him from the outside world. Perhaps the setting of the session which Kim’s therapist used affected his drawing. For instance exposing Kim to the artworks of her previous clients maybe influenced him to prove himself as more interesting and more willing to communicate certain unconscious feelings.
“Working within a therapeutic relationship is a private experience” (Dalley, 2013). A question I ask myself which relates to the field of art therapy and psychotherapy but not necessarily focusing on the topic of the therapeutic framework is the following “If the therapy experience is a private experience those that mean that that art therapist should not share her past clients work?” Isn’t showing past clients work breaking the framework of confidentiality? Considering the “wounded healer concept”, that a therapist is more perceptive at understanding others who suffered if they suffered themselves. If therapist cannot use their own personal stories of suffering to avoid breaking the therapeutic alliance what if the therapist’s past suffering is the same as the client’s current suffering could devolving their own personal experience still ruin the therapeutic alliance if their advice could benefit the patient?
References
Cabaniss, D.L., Cherry, S., Douglas. C.J., & Schwartz, A. (2011). Psychodynamic psychotherapy: A clinical manual. Hoboken, NJ: John Wiley & Sons. (chapters 1 & 8).
Dalley, T., Rifkind, G., & Terry, K. (2013). Three voices of art therapy: Image, client, therapist. London, UK: Routledge.
By Sinthia Cousineau
The psychodynamic theory focuses primarily on unlocking the past or the unconscious mind of the patient. Psychotherapy is therefore a form of treatment that aims to understand a patient’s unconscious, a concept originated by Freud who aimed to create a form a treatment that involves talking with a trained professional, hence the therapist. Cabaniss (2011) describes this understanding of the unconscious as “understanding what lies beneath the surface”. Once a patient understands and is made aware of their unconscious Cabaniss describes this as “uncovering”. For this to happen, the art therapist should establish an appropriate therapeutic frame for the psychotherapy, to allow the therapist to “separate what goes on in the therapy from what goes on outside” (Cabaniss, 2011, p.73). Art therapy is a field that uses art materials within the framework of a psychotherapeutic relationship. An art therapist uses the images that the patient produced to explore the unconscious of the patient for it allows the patient to focus on the issues and concerns that led them to start therapy (Dalley, 2013). This paper focuses on what constitutes the therapeutic frame in the field of psychotherapy and art therapy as well as describe why the establishment of the therapeutic frame is essential to this type of therapy. This is important because the therapy space is a place in which the patient will reveal their emotions, pain, vulnerabilities and personal tragedies. Hence, it is important for the patient to feel they are in a safe place to allow them to explore their unconscious mind and relive these emotions and painful childhood memories associated to these emotions. That is why patients need to be assured of the safety of the therapeutic setting (Cabaniss, 2011, p.73).
Cabaniss (2011) describes the therapeutic frame as being essential to the psychotherapy practice because it establishes a boundary for the therapist and patient as well as setting up a safe relationship for the patient. It also establishes a contract for the treatment that gives an idea of what to expect from the psychotherapy (Cabaniss, 2010). She describes how the frame of psychotherapy incorporates many different aspects such as the following: roles, time, setting, money, contact information, what to do in the event of an emergency, rules of confidentiality and issues related to supervision if the session is held by a therapist in training. Mainly Cabaniss focuses on how the frame of psychotherapy’s main purpose is to set a boundary which determines the appropriate behavior for therapist and patient. She describes it as being essential that that therapeutic frame be established at the start of therapy to help establish that boundary. She states that elements of the frame of psychotherapy should be considered the “ground rules” of psychotherapy. She also describes the two types of boundaries in psychotherapy. The first one is "boundary crossing which Cabaniss defines as a “deviation from the frame that may advance treatment and doesn’t harm the patient”. The second is boundary violation, which is “a deviation from the frame that is harmful or exploitative to the patient” (Cabaniss, 2011, p.72). This last one could be avoided by actively creating a frame with the patient.
The establishment of a therapeutic frame is essential to psychotherapy because it separates the outside world from what goes on in therapy, which enables the client to be assured they are in a safe space. Cabaniss (2011) also states that it allows a standard way for all patients meaning that each patient will be treated with the same elements of the therapeutic frame hence the same environment for their art making, the same rules of the patient-therapist relationship apply, and same boundaries. Role, a crucial element of the therapeutic frame is described as a part or function that a person plays in a particular situation. Cabaniss (2011). The role has two different parts: function and responsibilities. These are different for the therapist and the patient, for example the role of the art therapist or any psychotherapist is to listen to the patient, be understanding and nonjudgmental as to create a safe space for the patient and to be reliable by always showing up on time or alerting patient if late. The role of the patient is to attend the sessions on time, pay for the sessions and speak and participate in these sessions. When setting the frame both therapist and patient acknowledge which behavior is not appropriate, such as physical contact between therapist and patient. The patient should also be made aware that harassing the therapist is inescapable while the therapist however should avoid answering personal question as not to reveal too much about themselves to their client. As too much personal information will change the therapeutic relationship. Theses boundaries allow the session to become a safe place in which thoughts and feelings are allowed to surface (Dalley, 2013, p.8). Another important element of the therapeutic frame is time. According to Cabaniss (2011), setting a time allows the therapist to protect their patient. It means setting a time for individual sessions, a schedule of sessions and an overall ideal as to the duration of the therapy itself. The time should be reasonable for both patient and therapist. A third element of the therapeutic frame and one of the more important ones is the setting of the therapy. According to Cabaniss it is essential that the setting be a place designed for psychotherapy such as a clinic room or private office. Having the therapy session at a Starbucks for instance is not a good idea because it would turn the session into a social interaction, when therapy itself should remain a professional agreement. The setting also plays a crucial role in protecting the triatic relationship of therapist, patient and psychotherapy because it allows a safe space for the client to explore their unconscious. Cabaniss (2011) emphasizes the important of a “comfortable setting” which is a place where the patient is not bombarded with the personal information of the therapist. For example an office filled with photos of the therapist’s family or vacation trips would not be suitable. Other elements of the therapeutic frame include money. For therapy is a professional agreement and the client pays for the service of a professional. If for instance a patient cannot afford therapy the therapist should try to help them find a therapeutic service they could afford. Knowing the budget of the patient would also help establish how many sessions they could afford. Another element is the confidentiality of contact information. According to Cabaniss (2011) there are two reasons why a patient may need to contact their therapist outside of their session, and those are in the event of an emergency or to convey information such as needing to change the time of the session. Cabaniss also recommends that therapist have a separate phone line for their practice as to avoid mixing their professional life with their personal life. Transference is a very important concept in psychotherapy. It is described by Dalley (2013) as feelings that originate from childhood experiences or memories onto the therapist. Art making allows a patient to relive these memories and feelings. Based on Dalley’s description of Kim’s experience with Gabriella, we can see this surface as Kim is reliving his earlier memories of his parent’s fighting and sister’s eating disorder and his distant brothers. Making unconscious processes conscious is very complex and is achieved through interpretation of an image. This is how the art therapist facilitates communication and exploration of the unconscious by allowing the patient to create and then interpret their work (Dalley, 2013, p. 10). For example when interpreting Kim’s drawing of himself repairing his car, we can see that he was shutting himself off from society as he drew himself with his back turned to us and the hood of his car shielding him from the outside world. Perhaps the setting of the session which Kim’s therapist used affected his drawing. For instance exposing Kim to the artworks of her previous clients maybe influenced him to prove himself as more interesting and more willing to communicate certain unconscious feelings.
“Working within a therapeutic relationship is a private experience” (Dalley, 2013). A question I ask myself which relates to the field of art therapy and psychotherapy but not necessarily focusing on the topic of the therapeutic framework is the following “If the therapy experience is a private experience those that mean that that art therapist should not share her past clients work?” Isn’t showing past clients work breaking the framework of confidentiality? Considering the “wounded healer concept”, that a therapist is more perceptive at understanding others who suffered if they suffered themselves. If therapist cannot use their own personal stories of suffering to avoid breaking the therapeutic alliance what if the therapist’s past suffering is the same as the client’s current suffering could devolving their own personal experience still ruin the therapeutic alliance if their advice could benefit the patient?
References
Cabaniss, D.L., Cherry, S., Douglas. C.J., & Schwartz, A. (2011). Psychodynamic psychotherapy: A clinical manual. Hoboken, NJ: John Wiley & Sons. (chapters 1 & 8).
Dalley, T., Rifkind, G., & Terry, K. (2013). Three voices of art therapy: Image, client, therapist. London, UK: Routledge.
Psychoanalytic Approach to Dream Interpretation
The world of psychoanalytic therapy would not exist today if it was not for its founder Sigmund Freud, a physicist who studied neurophysiology. He was an Austrian who developed a method for treating psychopathology through conversation between a patient and a therapist. His goal was to discover the hidden world or the unconscious mind. Freud introduced his theory of the unconscious in his book titled “The Interpretation of Dreams” published in 1899. He developed the theory of the unconscious and divides the mind into three psychic structures known today as the id, ego, and super ego. He also developed the therapeutic techniques and concepts that are still implemented in therapy today, such as the use of free association, free-floating attention and transference. He was also popular for his interest in how sexuality affects one’s mind in particular how the sex drive can affect the death drive. In regards to this paper, we are particularly interested in his contributions to dream interpretations towards uncovering the unconscious mind.
Psychoanalysis was born in the city of Vienna, and Freud studied in the University of Vienna. This city of Vienna was once known as “die alte kaiserstadt” which meant the old imperial city. It was after the Prussians defeated France in 1870 that Berlin would replace Vienna as the center of the German-speaking world. After this defeat, Vienna would turn to denial as a kind of defense, and would focus more on mental illness then the world itself: “External reality is discounted and all mental energy is turned inward” only the inner life of the individual is allowed to matter. Vienna was one of the first city who was interested in the study of mental illness, but Freud is given credit as the founder of psychotherapy which is a form of treatment that aims to understand a patient’s unconscious, a concept originated by Freud who aimed to create a form a treatment that involves talking with a trained professional, hence the therapist (Bettleheim, 1990). This paper will focus on Freud’s psychoanalytic technique and how it relates to the unlocking of the unconscious mind through the interpretation of dreams.
Dreams according to Freud are extremely important when it comes to exploring the unconscious mind. He was not the only contributor to the field of psychology that was interested in dreams. Carl Rogers was reputed to record his own dreams. He stated that “While dreaming, the whole organism is undergoing a process of self-healing, similar to therapy”. Rogers believed the awareness of a dream is one aspect of a fully functioning person. Carl Jung believed that dreams compensate for one-sided feelings borne in consciousness. Feud however believed that dreams where means through which one’s unconscious wishes are expressed. He states that dreams were a way the unconscious processed unsatisfied wishes.
Koch (2012) believed that a dream is a process of nightly “self-healing, or nightly “psychological adjustment”’. She believed that most people remember their dreams in a time of crisis. For example people who are undergoing a divorce or loss of a loved one are more likely to remember their dream. Koch focused more on a person-centered approach to dreams, and states that we should focus more on what goes on in the clients mind and not solely on the therapist’s interpretation. She elaborates on the concept of lucid dreaming which is described as “when the dreamer knows she is dreaming while dreaming and can influence her dreaming process in a more active way”. She believes lucid dreaming to be an issue that may affect the relationship between the dream experience and the consciousness. She believes a dream is a congruent expression of the dreamer’s own experience and symbolization. Sharing a dream within a therapeutic setting allows the dream to become a narrative, and allows a further shift in meaning. She states that “dream conversations” can be of considerable significance to the therapeutic process and aid in each individual’s quest for meaning and self-understanding as well as providing insight into the patient’s inner world (Koch, 2012). Koch’s research has shown that people tend to experience dreams in a more intense way when dealing with life situations where persons are more prone to seek counseling or therapeutic help. There are different types of dreams that require the attention of therapy in particular, and these are: particularly vivid or salient dreams, troubling dreams, recurrent dreams, nightmares, or sleep terrors. We can use these dreams to increase our understanding of problems and make changes in to fix these problems. This will be discussed later in the paper when we focus on existential art therapy.
In 1899 Freud published his famous book titled “The Interpretation of Dreams”, where he introduces his theory of the unconscious in relation to dream interpretation and also discusses what will later develop into the theory of the Oedipus complex. “The interpretation of dreams is the royal road to knowledge of the unconscious activities of the mind” (Freud, 1900). Freud developed a theory that states that dreams are formed by two mental processes. The first is the unconscious forces that construct a wish that is expressed by the dream. The second process is the censorship that forcibly distorts the expression of the wish. He describes the latent content of a dream as the underlying meaning of the dream. Freud states that during sleep, the unconscious condenses, displaces, and forms representations of the dream content, the latent content of which is often unrecognizable to the individual upon waking Freud believed that the goal of a dream is to be satisfied of a repressed wish, he therefore treated dreams like a language to be deciphered. Freud describes that to understand the meaning of a dream you have to explore both the manifest content which is what the dream tells and the latent content which as previously mentioned is the concealed meaning of a dream (Freud, 1900).
Psychodynamic theory mainly focuses on treating the patient by exploring their unconscious mind. Cabaniss (2011) describes this as the as “understanding what lies beneath the surface”. Cabaniss emphasizes that in order for dreams to be understood there has to be a strong therapeutic alliance between client and patient. The patient needs to feel safe within the therapeutic setting. For this to happen, the art therapist should establish an appropriate therapeutic frame for the psychotherapy, to allow the therapist to “separate what goes on in the therapy from what goes on outside” (Cabaniss, 2011, p.73). Regarding the understanding of dreams, Cabaniss states “it’s a distortion to think that we ever know what a dream means, all we know is that dreams emerge from the unconscious mind and can thus help us learn about thoughts and feelings that are out of our awareness” (Cabanisset al., p. 259). To encourage the free association of the client about their dreams, Cabaniss suggest the use of techniques involving ambient listening, to begin reflecting an filtering and focusing on our listening. Cabaniss suggest that to better understand dreams one must focus on the following: What came before the report of the dream? What came after the report of the dream? At what point in the session was the dream reported? What words in the dream seem related to material surrounding the dream? As well as themes and concepts in the dream that seem related.
When it concern reflecting on dreams, Cabaniss (2011) describes three important concepts that help in the interpretation of dreams. These concepts are condensation, displacement and symbolization. Condensation is when two elements in the unconscious combine to work a single dream element. For example: I had a dream about a man, he looked like my ex-boyfriend, but he also kind of looked like a photo of my dad in college. Condensation is when several images are presented by a single image. Displacement is when one element in the manifest dream stands for something in the latent dream. For example a man had a dream before an important medical test. When he reports the dream he said “I had a dream last night about being late for my exam”. It is thus something represented by something else. Symbolization is described as an element in the manifest dream that symbolizes something in the latent dream, such as a person, wish, thought or idea. It is the transformation of latent thoughts into visual elements. Dream-work is composed of these three operations. Dreams are also composed of day’s residue, which are memory traces left by the events and psychic processes of the waking state; they are used as raw material by the dream-work that serves the wishes of the dreamer (Cabaniss, 2011).
Dreams interpretation is greatly aided by art. Freud stated that “It is not without reason that we speak of the power of art as magic” (Freud, 1913). He believed that the interpretation of dreams is the royal road to the knowledge of the unconscious activities of the mind. The dream is an unconscious signal and art therapy is also unconscious projection. If the client cannot build up the good quality relationship with the therapist, the client will not explore their unconscious dream by art therapy (Chu, 2014.) Art therapy therefore is incredibly useful in understanding the unconscious mind through dreams. Chu (2014) states that dream work applying in art therapy is helpful for emotion release, self-empowerment and self-acceptance and describes the art therapy process as having three roles: the role of the art therapist, the role of the client and the role of the artwork. The role of the therapist in this situation is to offer the client an environment to explore their dream status and art material without any words in the therapy process. The client has the role of using the art materials to touch the dream and then feel the flow of emotions and then reframe the meaning of the dream. The artwork also has a role, it allows a visual form for the dream to facilitate therapeutic relationship (Chu, 2014).
With regards to the topic of dreams, there are several art therapy interventions that can be applied. The most popular of these interventions is existential art therapy. Moon (2007) describes existential art therapy as a journey of self-discovery that is shared between the client and art therapist. The goal of this form of art therapy is to search for meaning, which is aided by the art therapist’s capacity to attend to the client. The ultimate goal is for the client to become an interpreter of their own dreams, and uses them to uncover a problem that needs to be fixed. Moon applies a metaphor to describe this type of art therapy intervention which he calls the “funnel metaphor”. The metaphor compares this type of art intervention to a funnel, because at each step of the process the client will filter and distill the content of their dream until a summary of statements of existential concern is identified and behavioral course of action is defined. Moon describes the various steps of this intervention, which can be broken down into twelve steps.
This intervention is mostly a dialogue between client and therapist. It is a process that helps clarify major issues in the lives of the client and helps them develop specific plans of action to respond to these problems and understand the messages their dream images present. The first step of the intervention involves the actual art making component which is the creation of the dream image. Once the dream image is completed the second step involves the client creating a written record known as the dream script. It is a basic explanation of what happens in the dream that is written down on paper. Step three is when the image is placed between the art therapist and the dreamer, and the dreamer reads his script out loud to the art therapist. Step four is similar to step tree but this time the art therapist reads the dreamer’s script out loud to the dreamer. Step 5 is a very important step in the procedure, it involves identifying the horizons in the dream. Moon (2007) describes horizons of a dream as the major words and phrases in the dream script that hold a particular important. In this step the art therapist asks the client to find and underline these words or phrases. The sixth step involves the amplification of the horizons. This is where the art therapist documents the client’s free association on the horizon. Free association is very important in Freudian approach to psychoanalytic therapy and cab be described as the mental process by which one word or image may spontaneously suggest another without any apparent connection. It is the expression of the content of consciousness without censorship as an aid in gaining access to unconscious processes. This technique is used in psychoanalysis as well as existential art therapy (Freud, 1900). The seventh step in the process is repeating the associations. The art therapist reads to the dreamer the notes that the dreamer recorded about their dream associations. Step eight involves clusting these horizons to find connections between them. Step nine involves the creation of existential statements of concern. The following step, is the summary of these statements of existential concern. The eleventh step is very important, it involves defining a course of action in response to the dream. The final step is committing to a course of action in response to the dream. In essence existential art therapy involves the dreamer filtering out his own free associations to the dream until he discovers the problem. In this type of art therapy intervention, the art therapist establishes a structure that serves strictly as a guide, recorder, and witness to the process, while the dreamer remains in control of each step of the process (Moon, 2007).
The world of psychoanalytic therapy would not exist today if it was not for its founder Sigmund Freud, a physicist who studied neurophysiology. He was an Austrian who developed a method for treating psychopathology through conversation between a patient and a therapist. His goal was to discover the hidden world or the unconscious mind. Freud introduced his theory of the unconscious in his book titled “The Interpretation of Dreams” published in 1899. He developed the theory of the unconscious and divides the mind into three psychic structures known today as the id, ego, and super ego. He also developed the therapeutic techniques and concepts that are still implemented in therapy today, such as the use of free association, free-floating attention and transference. He was also popular for his interest in how sexuality affects one’s mind in particular how the sex drive can affect the death drive. In regards to this paper, we are particularly interested in his contributions to dream interpretations towards uncovering the unconscious mind.
Psychoanalysis was born in the city of Vienna, and Freud studied in the University of Vienna. This city of Vienna was once known as “die alte kaiserstadt” which meant the old imperial city. It was after the Prussians defeated France in 1870 that Berlin would replace Vienna as the center of the German-speaking world. After this defeat, Vienna would turn to denial as a kind of defense, and would focus more on mental illness then the world itself: “External reality is discounted and all mental energy is turned inward” only the inner life of the individual is allowed to matter. Vienna was one of the first city who was interested in the study of mental illness, but Freud is given credit as the founder of psychotherapy which is a form of treatment that aims to understand a patient’s unconscious, a concept originated by Freud who aimed to create a form a treatment that involves talking with a trained professional, hence the therapist (Bettleheim, 1990). This paper will focus on Freud’s psychoanalytic technique and how it relates to the unlocking of the unconscious mind through the interpretation of dreams.
Dreams according to Freud are extremely important when it comes to exploring the unconscious mind. He was not the only contributor to the field of psychology that was interested in dreams. Carl Rogers was reputed to record his own dreams. He stated that “While dreaming, the whole organism is undergoing a process of self-healing, similar to therapy”. Rogers believed the awareness of a dream is one aspect of a fully functioning person. Carl Jung believed that dreams compensate for one-sided feelings borne in consciousness. Feud however believed that dreams where means through which one’s unconscious wishes are expressed. He states that dreams were a way the unconscious processed unsatisfied wishes.
Koch (2012) believed that a dream is a process of nightly “self-healing, or nightly “psychological adjustment”’. She believed that most people remember their dreams in a time of crisis. For example people who are undergoing a divorce or loss of a loved one are more likely to remember their dream. Koch focused more on a person-centered approach to dreams, and states that we should focus more on what goes on in the clients mind and not solely on the therapist’s interpretation. She elaborates on the concept of lucid dreaming which is described as “when the dreamer knows she is dreaming while dreaming and can influence her dreaming process in a more active way”. She believes lucid dreaming to be an issue that may affect the relationship between the dream experience and the consciousness. She believes a dream is a congruent expression of the dreamer’s own experience and symbolization. Sharing a dream within a therapeutic setting allows the dream to become a narrative, and allows a further shift in meaning. She states that “dream conversations” can be of considerable significance to the therapeutic process and aid in each individual’s quest for meaning and self-understanding as well as providing insight into the patient’s inner world (Koch, 2012). Koch’s research has shown that people tend to experience dreams in a more intense way when dealing with life situations where persons are more prone to seek counseling or therapeutic help. There are different types of dreams that require the attention of therapy in particular, and these are: particularly vivid or salient dreams, troubling dreams, recurrent dreams, nightmares, or sleep terrors. We can use these dreams to increase our understanding of problems and make changes in to fix these problems. This will be discussed later in the paper when we focus on existential art therapy.
In 1899 Freud published his famous book titled “The Interpretation of Dreams”, where he introduces his theory of the unconscious in relation to dream interpretation and also discusses what will later develop into the theory of the Oedipus complex. “The interpretation of dreams is the royal road to knowledge of the unconscious activities of the mind” (Freud, 1900). Freud developed a theory that states that dreams are formed by two mental processes. The first is the unconscious forces that construct a wish that is expressed by the dream. The second process is the censorship that forcibly distorts the expression of the wish. He describes the latent content of a dream as the underlying meaning of the dream. Freud states that during sleep, the unconscious condenses, displaces, and forms representations of the dream content, the latent content of which is often unrecognizable to the individual upon waking Freud believed that the goal of a dream is to be satisfied of a repressed wish, he therefore treated dreams like a language to be deciphered. Freud describes that to understand the meaning of a dream you have to explore both the manifest content which is what the dream tells and the latent content which as previously mentioned is the concealed meaning of a dream (Freud, 1900).
Psychodynamic theory mainly focuses on treating the patient by exploring their unconscious mind. Cabaniss (2011) describes this as the as “understanding what lies beneath the surface”. Cabaniss emphasizes that in order for dreams to be understood there has to be a strong therapeutic alliance between client and patient. The patient needs to feel safe within the therapeutic setting. For this to happen, the art therapist should establish an appropriate therapeutic frame for the psychotherapy, to allow the therapist to “separate what goes on in the therapy from what goes on outside” (Cabaniss, 2011, p.73). Regarding the understanding of dreams, Cabaniss states “it’s a distortion to think that we ever know what a dream means, all we know is that dreams emerge from the unconscious mind and can thus help us learn about thoughts and feelings that are out of our awareness” (Cabanisset al., p. 259). To encourage the free association of the client about their dreams, Cabaniss suggest the use of techniques involving ambient listening, to begin reflecting an filtering and focusing on our listening. Cabaniss suggest that to better understand dreams one must focus on the following: What came before the report of the dream? What came after the report of the dream? At what point in the session was the dream reported? What words in the dream seem related to material surrounding the dream? As well as themes and concepts in the dream that seem related.
When it concern reflecting on dreams, Cabaniss (2011) describes three important concepts that help in the interpretation of dreams. These concepts are condensation, displacement and symbolization. Condensation is when two elements in the unconscious combine to work a single dream element. For example: I had a dream about a man, he looked like my ex-boyfriend, but he also kind of looked like a photo of my dad in college. Condensation is when several images are presented by a single image. Displacement is when one element in the manifest dream stands for something in the latent dream. For example a man had a dream before an important medical test. When he reports the dream he said “I had a dream last night about being late for my exam”. It is thus something represented by something else. Symbolization is described as an element in the manifest dream that symbolizes something in the latent dream, such as a person, wish, thought or idea. It is the transformation of latent thoughts into visual elements. Dream-work is composed of these three operations. Dreams are also composed of day’s residue, which are memory traces left by the events and psychic processes of the waking state; they are used as raw material by the dream-work that serves the wishes of the dreamer (Cabaniss, 2011).
Dreams interpretation is greatly aided by art. Freud stated that “It is not without reason that we speak of the power of art as magic” (Freud, 1913). He believed that the interpretation of dreams is the royal road to the knowledge of the unconscious activities of the mind. The dream is an unconscious signal and art therapy is also unconscious projection. If the client cannot build up the good quality relationship with the therapist, the client will not explore their unconscious dream by art therapy (Chu, 2014.) Art therapy therefore is incredibly useful in understanding the unconscious mind through dreams. Chu (2014) states that dream work applying in art therapy is helpful for emotion release, self-empowerment and self-acceptance and describes the art therapy process as having three roles: the role of the art therapist, the role of the client and the role of the artwork. The role of the therapist in this situation is to offer the client an environment to explore their dream status and art material without any words in the therapy process. The client has the role of using the art materials to touch the dream and then feel the flow of emotions and then reframe the meaning of the dream. The artwork also has a role, it allows a visual form for the dream to facilitate therapeutic relationship (Chu, 2014).
With regards to the topic of dreams, there are several art therapy interventions that can be applied. The most popular of these interventions is existential art therapy. Moon (2007) describes existential art therapy as a journey of self-discovery that is shared between the client and art therapist. The goal of this form of art therapy is to search for meaning, which is aided by the art therapist’s capacity to attend to the client. The ultimate goal is for the client to become an interpreter of their own dreams, and uses them to uncover a problem that needs to be fixed. Moon applies a metaphor to describe this type of art therapy intervention which he calls the “funnel metaphor”. The metaphor compares this type of art intervention to a funnel, because at each step of the process the client will filter and distill the content of their dream until a summary of statements of existential concern is identified and behavioral course of action is defined. Moon describes the various steps of this intervention, which can be broken down into twelve steps.
This intervention is mostly a dialogue between client and therapist. It is a process that helps clarify major issues in the lives of the client and helps them develop specific plans of action to respond to these problems and understand the messages their dream images present. The first step of the intervention involves the actual art making component which is the creation of the dream image. Once the dream image is completed the second step involves the client creating a written record known as the dream script. It is a basic explanation of what happens in the dream that is written down on paper. Step three is when the image is placed between the art therapist and the dreamer, and the dreamer reads his script out loud to the art therapist. Step four is similar to step tree but this time the art therapist reads the dreamer’s script out loud to the dreamer. Step 5 is a very important step in the procedure, it involves identifying the horizons in the dream. Moon (2007) describes horizons of a dream as the major words and phrases in the dream script that hold a particular important. In this step the art therapist asks the client to find and underline these words or phrases. The sixth step involves the amplification of the horizons. This is where the art therapist documents the client’s free association on the horizon. Free association is very important in Freudian approach to psychoanalytic therapy and cab be described as the mental process by which one word or image may spontaneously suggest another without any apparent connection. It is the expression of the content of consciousness without censorship as an aid in gaining access to unconscious processes. This technique is used in psychoanalysis as well as existential art therapy (Freud, 1900). The seventh step in the process is repeating the associations. The art therapist reads to the dreamer the notes that the dreamer recorded about their dream associations. Step eight involves clusting these horizons to find connections between them. Step nine involves the creation of existential statements of concern. The following step, is the summary of these statements of existential concern. The eleventh step is very important, it involves defining a course of action in response to the dream. The final step is committing to a course of action in response to the dream. In essence existential art therapy involves the dreamer filtering out his own free associations to the dream until he discovers the problem. In this type of art therapy intervention, the art therapist establishes a structure that serves strictly as a guide, recorder, and witness to the process, while the dreamer remains in control of each step of the process (Moon, 2007).
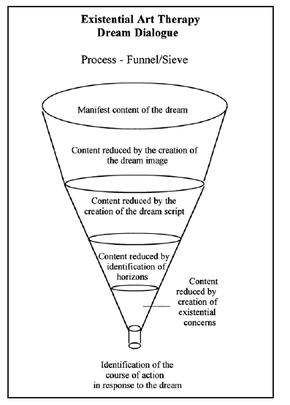
Figure 1: “The Funnel Metaphor for Existential Art Therapy”
According to Moon (2007) there are three premises that guide the existential art therapist’s interactions with the dreamer and their artwork, these are: the dream is what it is as there are no hidden meaning, the art therapist focuses on the manifest content of the images of the dream and client’s artwork and the art therapist refrains from making interpretive comments. Moon states that “through the process of interacting with and analyzing dream images, the existential art therapist attends to the dreamer by doing with, being open to, and honoring the dreamer’s struggles”. In existential art therapy, it is important that all interpretations of the artwork be left to the client. The role of the art therapist is to refrain entirely from interpretation of the client’s artwork or dream content, but rather guide the client to their own interpretations.
Of course this can be a struggle for an art therapist, for they may feel a desire to share their own interpretations with the clients. However it does benefit the clients to learn to form their own free associations and discover the problems on their own. When it concerns dreams, the major limitation is that only the dreamer can see their own dream, the therapist does not get to live the dream except online in the client’s descriptive narrative of the dream. This type of art intervention would be ideal for any client who suffers from trauma, for dreams then to happen more to those who suffered traumatic life events. It could also be applied to a population suffering for anxiety and phobias.
For my own personal reflection about this type of art intervention I decided to do the activity myself playing both the role of the art therapist and the client. I decided to focus on a recurring nightmare I often have. I decided to be an artwork based on watercolor, because it’s symbolic as watercolor is a very vivid and lose medium and dissolves easily like dreams do once you wake up. I took over thirty minutes to complete the artwork, as I try to consider that in an actual therapeutic session the client would have approximately that amount of time to create an artwork. The struggle for me was to think of a good idea for a dream, one that could potentially lead to an existential concern. I decided to pick one of my most recurrent nightmares which I had experienced over the years. In this nightmare I wake up and gradually lose all my teeth. So in the artwork I painted myself waking up and gradually having all my teeth fall off one by one.
Of course this can be a struggle for an art therapist, for they may feel a desire to share their own interpretations with the clients. However it does benefit the clients to learn to form their own free associations and discover the problems on their own. When it concerns dreams, the major limitation is that only the dreamer can see their own dream, the therapist does not get to live the dream except online in the client’s descriptive narrative of the dream. This type of art intervention would be ideal for any client who suffers from trauma, for dreams then to happen more to those who suffered traumatic life events. It could also be applied to a population suffering for anxiety and phobias.
For my own personal reflection about this type of art intervention I decided to do the activity myself playing both the role of the art therapist and the client. I decided to focus on a recurring nightmare I often have. I decided to be an artwork based on watercolor, because it’s symbolic as watercolor is a very vivid and lose medium and dissolves easily like dreams do once you wake up. I took over thirty minutes to complete the artwork, as I try to consider that in an actual therapeutic session the client would have approximately that amount of time to create an artwork. The struggle for me was to think of a good idea for a dream, one that could potentially lead to an existential concern. I decided to pick one of my most recurrent nightmares which I had experienced over the years. In this nightmare I wake up and gradually lose all my teeth. So in the artwork I painted myself waking up and gradually having all my teeth fall off one by one.

Figure 2: “My Artwork: losing all my teeth”
Once the artwork was completed I typed up a script about the dream. The following is my dream script: “In one of my most recurring dreams, I wake up or had recently woken up. I take my hand and touch my teeth lightly because I feel something strange. As I touch my teeth I can feel one of them is slightly loose, and then I touch my other teeth and feel more teeth are getting loose. Then the first tooth I touch gets very loose. Eventually more and more of my teeth get lose and I panic with the feeling I cannot control. Then my first took falls off entirely, and then the more I touch my teeth the more they all start to fall out. In the dream I panic and feel a lot of stress due to the sense that I cannot control my teeth falling out or the urge to keep touching them.”
The challenge for me was not the artwork itself but following all the steps to discover my own dream horizons and existential problems. I distilled all my free associations until I discovered that most of my free associations were related to anxiety and a fear of losing something. I discovered that my own existential statement of concern was that I feared losing control of myself through failure and anxiety.
I found that applying this art therapy intervention to myself was very useful towards understanding its complexity and the many different steps I had to implement. The major challenge for me was not to make my own interpretations when I played role of art therapist. I discovered how free association is very important in the psychoanalytic procedure. On a personal level it helped me gain a better understanding of myself as well as a better understanding of this art therapy technique. I would definitely love to continue learning more on this subject to perhaps focus more on fears and phobias and implement this intervention more with victims of trauma. This type of population is more likely to dream more symbolic dreams and remember them, which makes them ideal for this type of intervention.
The topic of dream interpretation in understanding trauma and fears is a fascinating topic I would certainly love to explore deeper one day.
The challenge for me was not the artwork itself but following all the steps to discover my own dream horizons and existential problems. I distilled all my free associations until I discovered that most of my free associations were related to anxiety and a fear of losing something. I discovered that my own existential statement of concern was that I feared losing control of myself through failure and anxiety.
I found that applying this art therapy intervention to myself was very useful towards understanding its complexity and the many different steps I had to implement. The major challenge for me was not to make my own interpretations when I played role of art therapist. I discovered how free association is very important in the psychoanalytic procedure. On a personal level it helped me gain a better understanding of myself as well as a better understanding of this art therapy technique. I would definitely love to continue learning more on this subject to perhaps focus more on fears and phobias and implement this intervention more with victims of trauma. This type of population is more likely to dream more symbolic dreams and remember them, which makes them ideal for this type of intervention.
The topic of dream interpretation in understanding trauma and fears is a fascinating topic I would certainly love to explore deeper one day.
References
Bettleheim, B. (1990). Freud’s Vienna. Freud’s Vienna and Other Essays (pp. 1-23). New York, NY: Knopft.
Cabaniss, D.L., Cherry, S., Douglas. C.J., & Schwartz, A. (2011). Psychodynamic Psychotherapy: A clinical manual. Hoboken, NJ: John Wiley & Sons. (chapters 1 & 8).
Chu, H. (2014). The Study of Therapeutic Effect of Hill’s Dream Work in Art Therapy. Procedia: Social and Behavioral Sciences 113, 68-73.
Freud, S. (1900). Interpretation of Dreams. The Standard edition of the complete psychological works of Sigmund Freud, James Strachery Ed., vol. 4 and 5. London, UK: Hodarth Press.
Koch, A. (2012). Situating Dreaming and Dreams in Person-Centered Theory and Practice: Cherishing client experiencing. Manchester, UK: Pccs Books.
Mitchell, S.A, & Black, M. J. (1995). Freud and beyond: A history of modern psychoanalytic thought. New York, NY: Basic Books.
Moon, B. (2007). Dialoguing with Dreams in Existential Art Therapy. Art Therapy: Journal of the American Art Therapy Association, 24 (3), 128-133.
Palombo, S.R. (2002). Theory of dreams. In E. Erwin (Ed.). The Freud encyclopedia: Theory, therapy, and culture(pp. 157-161). London, UK: Routledge.
Bettleheim, B. (1990). Freud’s Vienna. Freud’s Vienna and Other Essays (pp. 1-23). New York, NY: Knopft.
Cabaniss, D.L., Cherry, S., Douglas. C.J., & Schwartz, A. (2011). Psychodynamic Psychotherapy: A clinical manual. Hoboken, NJ: John Wiley & Sons. (chapters 1 & 8).
Chu, H. (2014). The Study of Therapeutic Effect of Hill’s Dream Work in Art Therapy. Procedia: Social and Behavioral Sciences 113, 68-73.
Freud, S. (1900). Interpretation of Dreams. The Standard edition of the complete psychological works of Sigmund Freud, James Strachery Ed., vol. 4 and 5. London, UK: Hodarth Press.
Koch, A. (2012). Situating Dreaming and Dreams in Person-Centered Theory and Practice: Cherishing client experiencing. Manchester, UK: Pccs Books.
Mitchell, S.A, & Black, M. J. (1995). Freud and beyond: A history of modern psychoanalytic thought. New York, NY: Basic Books.
Moon, B. (2007). Dialoguing with Dreams in Existential Art Therapy. Art Therapy: Journal of the American Art Therapy Association, 24 (3), 128-133.
Palombo, S.R. (2002). Theory of dreams. In E. Erwin (Ed.). The Freud encyclopedia: Theory, therapy, and culture(pp. 157-161). London, UK: Routledge.
| viennese_culture_and_its_psychological_complexities.docx |
| psychoanalytic_approach_to_dream_interpretation.pdf |
| freudian_psychoanalytic_theory.pptx |